
Fertility Preservation Options Before Cancer Therapy
A cancer diagnosis shouldn’t stop you from considering growing your family. Our expert and trustworthy doctors are here to help with fertility preservation techniques that are safe and successful. You can feel confident that your family plans are still within reach.
In Vitro Fertilization (IVF) & Embryo Banking
Embryo banking is the most established form of fertility preservation and is a wonderful option for women who have a male partner or those interested in using donor sperm.
The process of IVF and embryo banking involves stimulating the ovaries to produce multiple eggs, combining these eggs with sperm in the laboratory, and freezing the embryos that result. IVF and embryo banking occur over 2-6 weeks. We then transfer one embryo at a later date after cancer treatment and recovery have been completed.
For breast cancer patients, we may employ specific ovarian stimulation protocols to reduce your exposure to estrogen.
Egg Banking
Egg (or “oocyte”) banking is similar to embryo banking because it involves the same hormonal stimulation of your ovaries to produce multiple eggs. Like embryo banking, we surgically retrieve the eggs from your ovaries and freeze them — but without being fertilized by sperm.
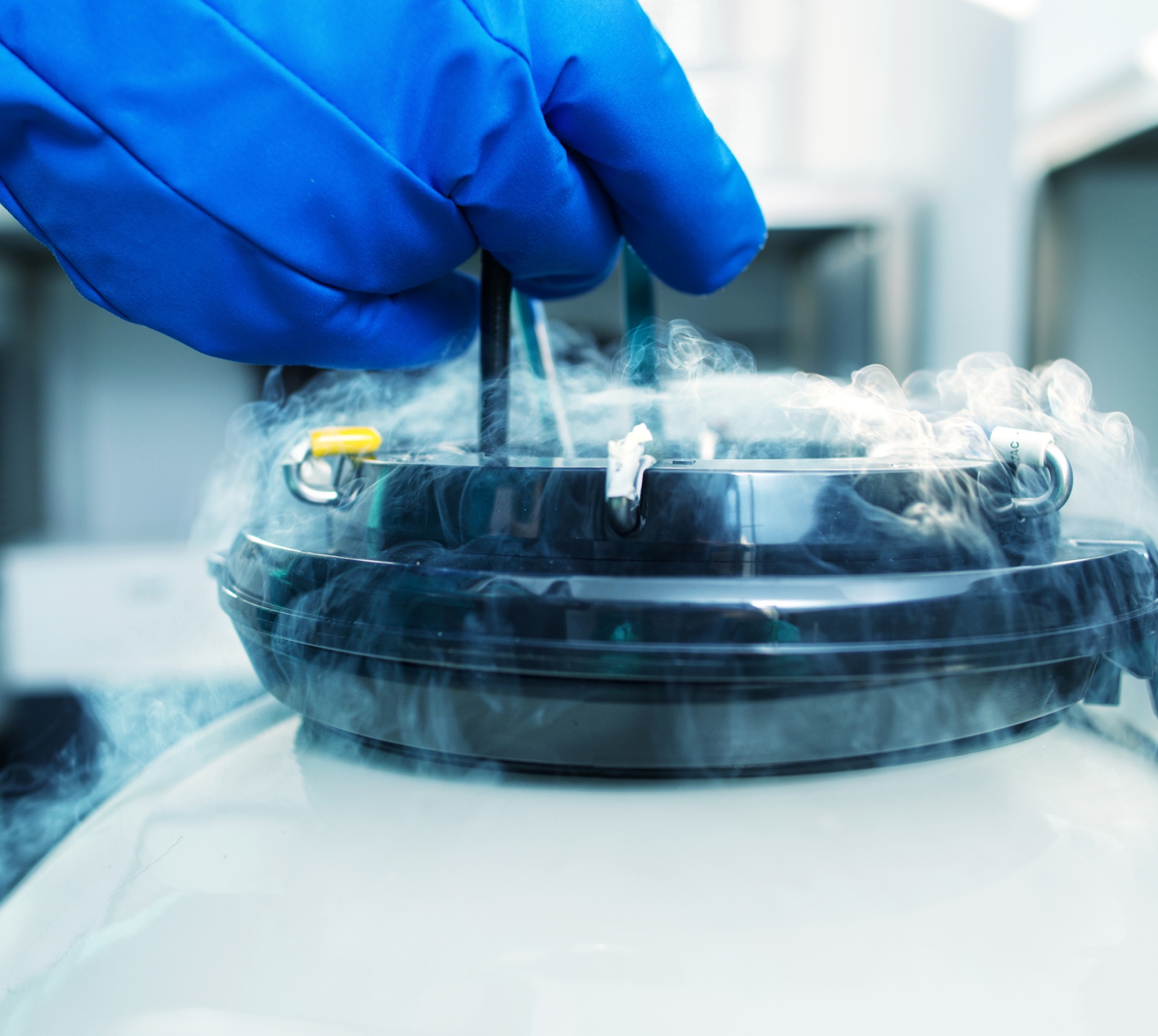
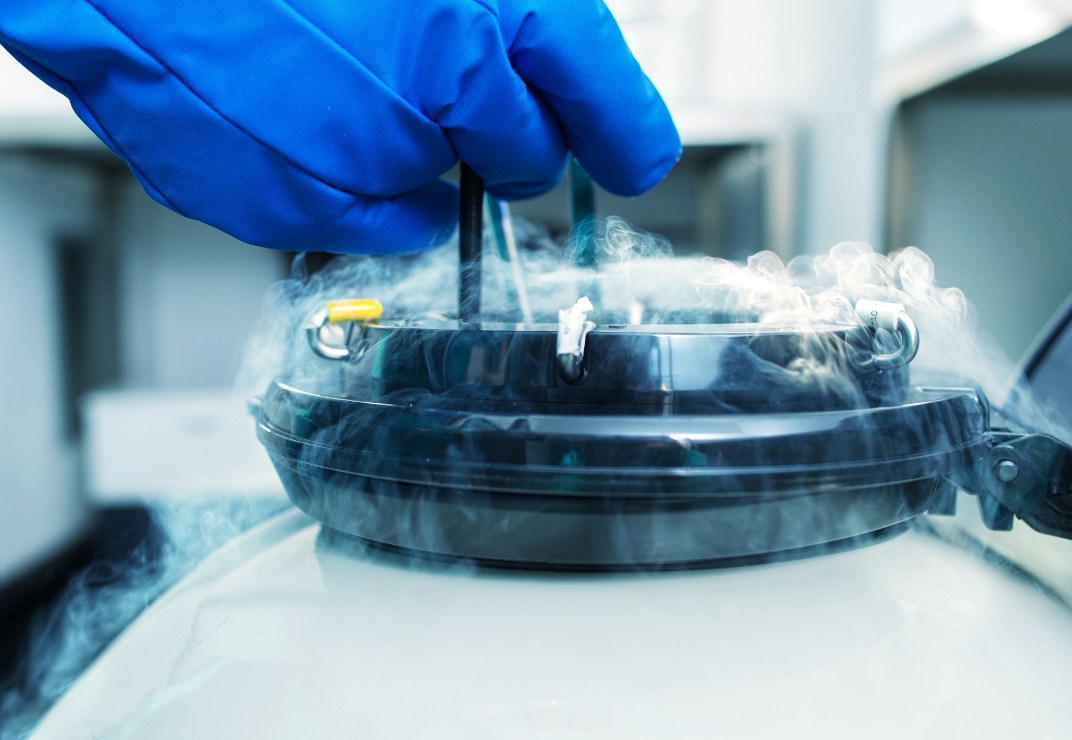
At RPSD, we specialize in an advanced cryopreservation technique called egg vitrification, or “rapid egg freezing.” During this process, your eggs are kept frozen in our laboratory until you’re ready to fertilize them (using sperm from your partner or a donor). Our skilled fertility doctors then transfer the resulting embryo(s) after you complete cancer treatment and recovery.
We recommend egg banking for:
- Women who do not have a male partner or are not interested in using donor sperm
- Women who can safely delay cancer treatment for 2-6 weeks

Ovarian Tissue Banking
Your doctor may recommend ovarian tissue banking if you do not wish to (or cannot safely) delay cancer treatment to undergo embryo or egg banking.
For ovarian tissue banking, your gynecologic oncologist will remove part of or the whole ovary through a minor surgical procedure called laparoscopy. The outer surface (cortex) of your ovary, which contains the eggs, is frozen in strips for later use.
Women who are survivors of certain types of cancer may have pieces of the tissue thawed and transplanted back. Many pregnancies have resulted from this technique. However, transplantation is not safe following some types of cancer (e.g., leukemia) because of the risk of re-seeding the original cancer.
We partner with the national Oncofertility Consortium®, an NIH-funded program actively researching new ways to use this tissue. Though this option is experimental, it may be best if your doctor recommends starting cancer treatment immediately.

Fertility Sparing Surgery
If you have been diagnosed with early-stage cervical or ovarian cancer, experienced gynecologic oncologists may be able to conserve your reproductive organs at the time of your cancer surgery. If your cancer treatment includes receiving abdominal or pelvic irradiation, it may be possible to surgically move your ovaries out of the radiation field (ovarian transposition).
We recommend fertility sparing surgery for:
- Women who will be exposed to abdominal or pelvic irradiation
- Women with early-stage cervical cancer

Your Fertility Treatment Options After Cancer
According to current research, depending on the specific cancer, pregnancy does not increase the risk of cancer recurrence, and children born to cancer survivors do not appear to be at a higher risk of birth defects. After completing your cancer therapy, our board-certified reproductive endocrinologists will tailor a fertility treatment plan to your unique needs. Common fertility treatments for cancer survivors include:





Stories from Our Patients
We’re honored to help patients achieve their dream of growing their families. Here are a few of their success stories.


Fertility Education Center


Fertility Treatments and Your Lifestyle
The lifestyle you lead directly affects your fertility. From making healthy lifestyle choices to supplementing your intake of important nutrients, here are some key steps you can take outside the clinic to improve and maintain your chances of becoming pregnant.
Let’s Take the Next Step Together
Our skilled fertility specialists are here to help. Contact us today and let’s discuss the next phase of your fertility journey.